
Rock Climbing and the Injuries that Make us Human
One of the most exhilarating activities Chattanooga offers can be one of the most physically demanding sports us humans engage in. Climbing in Tennessee challenges every muscle in the body and sometimes results in climbing injuries. Be it elbow tendonitis, pulling too hard for too long, or the dreaded pully system tear. I’m going to break down the most common climbing injuries over the next few articles and discuss how visiting a Chattanooga sports chiropractor will help you heal and perform better at the crag.
This series is designed to give you a better understanding of climbing shoulder anatomy, shoulder injuries, and ways to climb better. We’ll specifically discuss shoulder pain, shoulder movement problems, and functional exercises to improve your climbing.
The shoulder complex is very mobile and allows you the flexibility to move your arms and position your body for difficult maneuvers. The shoulder is a ball and socket joint (humerus fits into the scapula) affording the arm 360 degrees of pain free movement. We’ll refer to this as your glenohumeral joint (GH).

Image credit: https://www.webmd.com/pain-management/picture-of-the-shoulder
Your rotator cuff muscles act to “suck” your humerus into the socket of the scapula (shoulder blade). The scapula is my favorite bone because it is not only funny looking, but it is so important. It is held down on the rib cage by a sling of muscles and positions the arm to achieve pain free motion. We’ll discuss this area as the scapulo-thoracic joint. The last bone we’ll discuss is your clavicle. It is the only spot your arm and scapula attaches bone on bone to your skeleton. If this is misaligned it will throw your entire shoulder off and is a common chiropractic adjustment of the shoulder. Scapulo-thoracic biomechanics need to be functionally sound to take the heat off the glenohumeral joint. If there is a movement error, your spine is misaligned, or you are fatigued you may compromise and over pull with incorrect movements leading to common shoulder issues.
Common shoulder injuries and how to prevent them
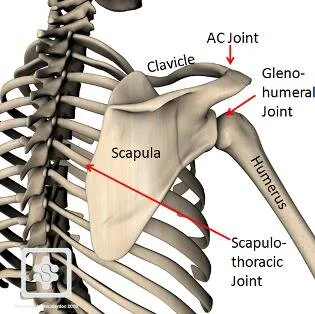
Image credit: https://www.physio-pedia.com/File:Scapulothoracic-joint.jpg
What is discussed below is not meant to be a diagnostic tool, however it should be educational. Proper assessment from a professional sports physician (sports chiropractor, physical therapist, osteopath) should be completed before you self-diagnose and self-treat. As a sports chiropractor specializing in athletes, it is my goal to complete a comprehensive functional movement assessment to help diagnose and treat your chief complaint by adjusting the spine and extremities, completing muscle and fascial release techniques, and apply movement reeducation therapies. The overarching mission is allowing you to return to climbing pain free with better biomechanics, decreasing your odds for future injuries.
Subacromial Impingement (shoulder impingement)
Pain on the outside of the shoulder and/or pain raising the shoulder over 90 degrees are common complaints. A test would be if there is pain raising the shoulder with your thumbs down, but no pain raising your shoulder with your thumbs up. Since there is a such a small space for your rotator cuff muscles to work, inflammation from overuse or improper biomechanics can manifest itself as impingement.
Rotator cuff strain / Rotator cuff tear
Dull aching on the back of your shoulder blade, weakness / discomfort / pain when lifting objects are common complaints with rotator cuff injuries. The rotator cuff acts to position the humerus in the socket, allowing the bigger muscles, biceps, lats, and pectoral muscles to achieve the big movements like doing pull-ups. Poor climbing posture will lead to increase stress on these muscles contributing to inflammation and possible tear or rupture if no correction of the climbing technique occurs.
Bicep tendinopathy / biceps tendon subluxation
Pain or discomfort with bending the elbow, rotating your wrist from palm down to palm up, or clicking of near your glenohumeral joint with shoulder movements. Climbing requires a lot of pulling, meaning your biceps are in overdrive the entire climb. This can lead to an overuse injury of biceps muscle and also increase its susceptibility to become subluxated or torn.
Scapular winging
Visualizing the lower point of the scapula coming off of the rib cage and sometimes coming off the back near the spine. This can be caused by weakness of scapular stabilizers (serratus anterior and lower trap mainly), nerve damage, AC joint separation to name a few. Without proper retraction and protraction of the scapula during climbing we can increase the odds of injuries elsewhere. This is one of the most important movement faults to correct.
Some other injuries include...
Labral tears, AC joint instability or separation, shoulder dislocation, and bursitis. Some of these require immediate medical attention and should not be procrastinated upon. Labral tears normally are accompanied by deep shoulder pain and possible clicking. Acromioclavicular separation is normally visualized by one collar bone sticking up higher asymmetrically than the other near the shoulder also accompanied by pain and limited mobility. A dislocated shoulder will normally show itself by a very painful and sometimes audible pop presenting as squared off shoulder.
Some specifics a sports medicine doctor will do are chiropractic adjustments to the spine, clavicle, AC joint, GH joint, and ribs. Shoulder cupping, kinesiotaping, and myofacisal release to surrounding areas as well. Shoulder stretching and functional rehab exercises will be taught to round out treatment.